
Abstract
Due to its advantages over open surgery and conventional laparoscopy, uptake of robot-assisted surgery has rapidly increased. It is important to know whether the existing open or laparoscopic skills of robotic novices shorten the robotic surgery learning curve, potentially reducing the amount of training required. This systematic review aims to assess psychomotor skill transfer to the robot in clinical and simulated settings. PubMed, EMBASE, Cochrane Library and Scopus databases were systematically searched in accordance with PRISMA guidelines from inception to August 2021 alongside website searching and citation chaining. Article screening, data extraction and quality assessment were undertaken by two independent reviewers. Outcomes included simulator performance metrics or in the case of clinical studies, peri- and post-operative metrics. Twenty-nine studies met the eligibility criteria. All studies were judged to be at high or moderate overall risk of bias. Results were narratively synthesised due to heterogeneity in study designs and outcome measures. Two of the three studies assessing open surgical skill transfer found evidence of successful skill transfer while nine of twenty-seven studies evaluating laparoscopic skill transfer found no evidence. Skill transfer from both modalities is most apparent when advanced robotic tasks are performed in the initial phase of the learning curve but quality and methodological limitations of the existing literature prevent definitive conclusions. The impact of incorporating laparoscopic simulation into robotic training curricula and on the cost effectiveness of training should be investigated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Robotic surgery has experienced a rapid increase in uptake, with a four-fold increase in the number of robot-assisted operations performed over the last decade [1]. The continuing favourability of robot-assisted surgery (RAS) is due to the numerous advantages it possesses over open surgery and conventional laparoscopy such as faster learning curves, eradication of the fulcrum effect and the ability to mirror the movements of the wrist and hand [2]. Furthermore, when compared to open procedures, RAS operations have resulted in more favourable patient-centred outcomes such as significantly decreased blood loss, length of hospital stay, transfusion rates [3] and lower post-operative pain medication use [4].
Therefore, as experienced surgeons switch to robot-assisted operations to capitalise on its advantages, it is now a priority to address the training needs of current and future surgeons. It is clinically important to know how far existing skills transfer for safe robot-assisted operations on patients, and whether prior open or laparoscopic experience complicates or complements the robotic skill acquisition process. There are also implications for surgical trainees undergoing robotic training, based solely on the acquisition of robot-specific technical skills. Simulation forms the initial stage of robotic skills training due to its convenience, efficiency and provision of safe training posing no risk to patients [5]. Robotic simulators are more expensive [6] and less available than laparoscopic simulators [7, 8], so establishing whether skills learnt on laparoscopic simulators transfer to the extent that less time is needed on robotic simulators may optimise the use of such limited resources.
It might be expected that open surgical experience translates into enhanced robot-assisted performances as knowledge of the anatomy and approaches associated with operating in a particular region may aid in mastering the robotic form of the operation. Similarly, given that laparoscopic surgeons are well versed in fundamental minimally invasive techniques and accustomed to manoeuvring instruments through an indirect field of view, they might be well equipped with transferable skills to augment their robotic skills. This review aims to assess the transfer of open and laparoscopic psychomotor skills (gained through surgical simulation or operative experience) to the robot, evaluating their impact on the robotic learning curve. Successful crossover of skills across the various modalities would not only result in surgeons being able to operate across a range of settings but may optimise their training in terms of duration and cost effectiveness.
Methods
Design
A systematic review assessing the transfer of open and laparoscopic skills to robotic surgery was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [9]. A review protocol was prospectively designed and registered on the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42021231235) [10].
Eligibility criteria
Studies involving medical students, surgical trainees and consultant surgeons (expert surgeons) were included, with exclusion of any study involving non-medical participants. Eligible interventions included assessed performances of robotic tasks or procedures after undergoing laparoscopic training or having prior laparoscopic or open surgical experience. Comparators included control participants (no open or laparoscopic experience) or robotically trained participants. Outcomes included measures of task performance in operative or simulated settings, with studies not assessing the impact of skill transfer in statistical terms being excluded. Randomised controlled trials, non-randomised comparative studies, cohort studies and observational studies evaluating skill transfer were included. Review articles, editorials, letters to the editor and conference abstracts were excluded. A restriction on language was imposed, with only studies written in English being included.
Search strategy
The PubMed, EMBASE, Cochrane Library and Scopus databases were systematically searched from their inception to August 2021. A combination of free-text terms and medical subject headings (MeSH) was used in the searches. For PubMed and the Cochrane Library, the search strategy ‘(laparoscop* OR open OR Laparoscopy[mesh] OR Minimally Invasive Surgical Procedures[mesh]) AND (robot* OR Robotic Surgical Procedures[mesh]) AND (transfer*)’ was used. For Embase, ‘((laparoscop* OR open) AND robot* AND transfer*)’ was used, while ‘((laparoscop* OR open) AND surg* AND robot* AND transfer*)’ was employed for Scopus. The Google Scholar search engine was employed in combination with website searching and citation chaining to find relevant grey literature.
Study selection and screening
Initial screening of article titles and abstracts was performed by two independent reviewers (BC and MSAA). Duplicates were removed and the full text of articles which passed this initial screening process was then assessed for eligibility against the inclusion criteria. Disagreements over inclusion or exclusion were referred to a third reviewer (AA).
Data extraction and risk of bias assessment
Data extraction was performed by two independent reviewers using a pre-defined, standardised form. Any disagreements were resolved by a third reviewer. Data extracted included study characteristics such as author, publication date, study type and study population, as well as study outcome measures and results. All included studies were assessed for risk of bias by two independent reviewers using the Cochrane risk-of-bias tool for randomised trials (RoB 2) [11] and the Risk Of Bias In Non-Randomised Studies of Interventions (ROBINS-I) tool [12]. Disagreement was resolved by referral to a third reviewer.
Data synthesis
It was not possible to undertake a meta-analysis due to heterogeneity in study design and outcome measures. Thus, results were narratively synthesised in accordance with PRISMA [9] and Synthesis without meta-analysis (SWiM) [13] guidelines.
Results
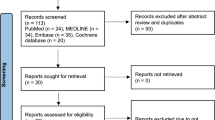
One thousand one hundred and fifty-two records were identified through database searching and fourteen additional records were identified through a search of the grey literature and citations. After deduplication, 693 studies were eligible for title and abstract screening with 622 studies being excluded, leaving 71 studies for full-text screening (Fig. 1). Forty-two studies were then excluded after full-text screening. Thus, 29 studies were included for narrative synthesis.

PRISMA flow diagram
Characteristics of included studies
The characteristics of the included studies are displayed in Tables 1 and 2. Of the studies included were 9 randomised controlled trials [20, 21, 23, 24, 27, 32, 33, 38, 42] (RCTs), 15 prospective cohort studies [15, 16, 22, 25, 26, 28,29,30,31, 34,35,36,37, 39, 41], 2 non-randomised controlled trials [18, 40], 1 retrospective cohort study [17], 1 uncontrolled before-and-after study [19] and 1 prospective single-surgeon study [14]. The publication dates of the included studies ranged from 2003 to 2020. All studies had a small sample size ranging from the results of 1 surgeon [14] to 21 participants [30]. Study participants included medical students, surgical trainees of all levels of training and expert surgeons. Robotic systems used in studies included the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA), the Mimic dV-Trainer (Mimic Technologies Inc., Seattle, Washington), the RoSS surgical simulator (Simulated Surgical Systems, Williamsville, New York) and the Senhance Surgical System (TransEnterix Inc., Morrisville, NC).
Risk of bias
The results of the risk of bias assessment are depicted in Appendices 1 and 2. Two studies were assessed to have low risk of bias [23, 38] while nineteen studies were judged to have some concerns over risk of bias. Eight studies were deemed to be at high overall risk of bias.
Findings
The heterogeneity in study design, participants, interventions and outcome measures prevented the undertaking of a meta-analysis so the results were narratively synthesised, categorised into the type of setting and then into either transfer of open skills or transfer of laparoscopic skills.
Real-time skills transfer
Four studies [14,15,16,17] evaluated skill transfer in the clinical setting (Table 3). One study [14] demonstrated the successful transfer of open skills to robotic prostatectomy, describing an experienced open surgeon (with robotic experience of a day’s training course and two cadaveric procedures) achieving a 4-h proficiency after just 12 patients. All outcomes were satisfactory and equivalent to the performances of ‘expert’ surgeons who had experience of over 100 robotic procedures.
Three studies [15,16,17] assessed the transfer of laparoscopic skills to robotic surgery in the clinical setting. Eddib et al. [15] evaluated robot-assisted laparoscopic hysterectomy performances with the only significant difference reported being that the advanced laparoscopic surgeons had a shorter mean procedure time (121 vs 174 min, p < 0.05) with comparable performances in all other metrics. Kilic et al. [16] also reported time reductions for laparoscopically trained participants, concluding that prior laparoscopic experience contributes to an improved robotic surgery learning curve in the context of vaginal cuff closure. In contrast, IK. Kim et al. [17] evaluated the first 100 robot-assisted rectal cancer resections performed by a highly experienced laparoscopic surgeon and a surgeon with limited laparoscopic experience, finding comparable results overall.
Simulated setting
Table 4 illustrates the findings of the studies assessing skill transfer in the simulated setting. Two studies [22, 30] assessed the transfer of open skills to robotic surgery, with both using the da Vinci Skills Simulator. Cumpanas et al.’s [22] cohort study found no significant difference in the overall performance of open surgeons and surgical novices on the basic robotic task of Peg Board (80 vs 78%, p = 0.5) but as task complexity increased, the open surgeons performed significantly better. Conversely Kowalewski et al. [30] found no significant differences in the performances of open surgical novices, intermediates and experts on the Peg Board, Pick and Place and Suture Sponge tasks, with novices outperforming experts on the Thread the Ring task.
Twenty-four studies [18,19,20,21, 23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] evaluated the transfer of laparoscopic skills to robotic surgery in the simulated setting. Thomaier et al. [38] assessed the performance of a basic robotic task (Peg Transfer) by surgical novices trained on either a laparoscopic or a robotic simulator, reporting that the laparoscopic trained group successfully transferred their skills to the robot with the mean time to complete the robotic task decreasing from baseline (167 vs 120 s, p = 0.004) with significant improvements in the global rating composite score and instrument collisions score. The transfer is incomplete, however, as the laparoscopic trained group were outperformed on the robotic platform by the robot trained group.
Three studies [24, 26, 35] reported successful skill transfer in both basic and advanced tasks. Hagen et al. [26] found that laparoscopically trained surgeons significantly outperformed laparoscopically naïve participants on ring placement, suturing with knot tying and needle guidance tasks, concluding that laparoscopic experience is a strong predictor of robotic performance. Feifer et al. [24] described significant performance improvements in all robotic tasks (Peg Transfer, Cutting, Intracorporeal Knot Tying and Cannulation) for surgical novices who had received dual training on augmented reality (ProMIS) and virtual reality (LapSim) laparoscopic simulators, with no significant improvements observed in those who had received no training and fewer significant improvements in participants who had trained on either simulator alone.
Ten studies [18, 19, 23, 25, 28, 29, 31,32,33,34] found that laparoscopic skill transfer was most evident when advanced surgical tasks such as intracorporeal knot tying or suturing were performed. In an RCT conducted by Davila et al. [23], the mean score improvement for robotic intracorporeal knot tying was greatest for inexperienced surgical trainees who had undergone 4 weeks of laparoscopic training compared to those who instead received 4 weeks of robotic training (82.2 vs 40.5 points, p = 0.018). In accordance with the findings of Davila et al., Panait et al.’s [34] cohort study reported that performances on the robot equalled those on the laparoscopic platform as the complexity of tasks increased thereby demonstrating transfer of skills.
Finnerty et al. [25] echoed these findings, reporting a statistically significant correlation between the number of laparoscopic operations logged by surgical trainees and performance on an advanced robotic task only (Suture Sponge) (p = 0.005, r2 = 0.21). Jayaraman et al.’s [28] study also reported that increased minimally invasive surgical experience correlated with a decreased likelihood of anastomotic leak when performing the complex task of suturing a biliary-enteric anastomosis in robotic choledochojejunostomies on a porcine model.
McVey et al.’s [31] cohort study found that baseline laparoscopic task time of surgical trainees on the advanced Intracorporeal Suturing with Knot Tying (ISKT) task, but not the basic Peg Transfer (PT) task, correlated with post-robotic training performances of both Peg Transfer and ISKT time. In a similar fashion, Moncayo et al. [32] described significant skill transfer for laparoscopically trained students to the confined space of the simulated paediatric robotic platform for the advanced Thread the Ring task (p = 0.01) but not for the basic Transfer the Plot task (p = 0.96). Obek et al. [33] evaluated the performances of laparoscopically trained students on the advanced knot tying robotic task, reporting that their composite score significantly increased after training (43% improvement, p = 0.02) with a significant decrease in error score (16.2 vs 42.1, p = 0.02) thereby demonstrating skill transfer to the robot.
In contrast, nine studies [20, 21, 27, 30, 36, 39,40,41,42] found no evidence of skill transfer in either basic or advanced tasks. Tillou et al.’s [39] study involved assessment of the more advanced task of suturing alongside basic tasks such as camera manipulation and Endowrist handling, finding comparable performances across all tasks between laparoscopically experienced surgeons and laparoscopically naïve trainees thereby signifying a complete lack of skill transfer. Similarly, Zihni et al. [42] found no evidence of laparoscopic skill transfer in both basic and advanced robotic tasks, noting that prior performance of the Pattern Cutting task on the laparoscopic platform appeared to impede subsequent performance of the task on the robot. Teishima et al. [37] reported significantly better overall Suture Sponge scores in the initial trials for laparoscopic experts compared to surgeons with less experience but by the fourth trial, there was no significant difference in scores (59.1 ± 19.5 vs 49.1 ± 7.0, p = 0.1068) suggesting that laparoscopic experience only confers an advantage in the initial phase of the robotic learning curve.
Discussion
Robotic training curricula consist of multiple modalities aiming to develop the necessary cognitive and psychomotor skills for safe robotic surgical practice. These modalities include dry and wet laboratory training, virtual reality simulation and online lectures [43]. Skill transfer from robotic virtual reality simulation to the operative environment has been demonstrated, thereby indicating its integral role in training curricula [44]. This review aimed to evaluate the presence of crossover from a trainee’s open or laparoscopic skills as any such skill transfer might accelerate the robotic training process and also result in greater availability of expensive robotic simulators to other trainees as less time is spent in the simulation phase. The results of the 29 included studies found conflicting evidence relating to the transfer of open and laparoscopic skills to robotic surgery in both clinical and simulated settings.
Successful open surgical skill transfer to the robotic clinical setting was demonstrated with satisfactory peri- and post-operative outcomes achieved in the absence of any laparoscopic experience [14]. However, the findings of the studies conducted in the simulated setting confirm the current view in surgical practice that open surgical skill transfer of any extent is insufficient in itself to enable a direct transition to robotic surgical practice in the absence of any systematic robotic training; one study found no evidence of any skill transfer [30] while the other reported skill transfer only for advanced robotic tasks [22].
Laparoscopic surgical experience only translates into reduced robotic procedure time in the clinical setting, with no significant improvement in other metrics [15, 16]. One study [17] contrarily reported that the surgeon with the least laparoscopic experience had a significantly shorter mean operative time but acknowledged confounders such as differing specimen extraction and anastomosis techniques between the surgeons which might have affected procedure time. Successful laparoscopic skill transfer does occur in the simulated setting, most notably when advanced robotic tasks are performed [37] although some studies did observe a transfer effect for basic tasks as well [23, 24, 26, 35, 38]. Substantial laparoscopic experience is not essential for successful skill transfer to occur as six studies [18, 19, 24, 32, 33, 38] reported a transfer effect in surgical novices following their completion of short laparoscopic training courses.
Thus, for both open and laparoscopic modalities, several studies suggested a possible correlation between task complexity and the extent of skill transfer. This is consistent with the high construct validity (ability to differentiate between experts and novices) associated with advanced robotic tasks such as Suture Sponge [45], so any superiority in the performances of open or laparoscopically experienced participants would be most evident in these tasks. Cumpanas et al. [22] attributed open surgeons’ extensive prior experience in guiding the needle from different angles when performing suturing as the reason for the transfer effect seen but noted that this inclination to reproduce their usual open surgery hand movements on the robotic console resulted in a worse master workspace score (a metric representing the virtual space used by the instruments during task performance). In contrast, Pimentel et al. [36] reported significantly better master workspace scores for laparoscopic surgeons as they are accustomed to manoeuvring instruments in a confined space which suggests that, unlike open surgical experience, prior laparoscopic experience enhances efficiency of movement on the robotic platform.
As described for open surgery [22], another reason for the laparoscopic transfer effect observed on advanced tasks may include an existing skillset of needle driving developed through repetitive practice and experience which predisposes laparoscopically trained participants to a more precise performance on the robot [25, 26, 29]. Two studies [24, 33] also conjectured that laparoscopic training facilitates the development of visual cues associating knot tension with suture resistance, thus preparing the participant for the loss of haptic feedback on the robotic platform but this is contrary to existing literature which reported that the perception of haptic feedback on the robot is similar between novices and laparoscopic surgeons [46].
There may be a preliminary period in which laparoscopically trained subjects transitioning to robotics adopt a conservatory strategy with camera and instrument movements [21] as they ‘unlearn’ certain laparoscopic-associated acquisitions [39] such as adjustment for the fulcrum effect [41] to adapt to the robotic console. This could explain why, for studies in which a progressively difficult task sequence was employed, performances improved as task complexity increased because the initial basic robotic tasks may serve to prime and enable modification of the laparoscopic skillset to the robot. This, therefore, implicates a role for systematic robotic training to include both basic and advanced tasks regardless of a surgeon’s prior laparoscopic experience.
Limitations
Limitations to the review findings include the low quality of certain studies, small sample sizes and low number of task repetitions assessed in some of the included studies. Reporting of outcomes also varied between studies, thus preventing a meta-analysis of results, with some studies electing to use time and score measurements only which precludes comprehensive assessment of surgical performance [47]. Confounders for laparoscopic skill transfer studies such as open surgical experience [22, 29] and video gaming experience [48] were inconsistently reported with variation in the definition of ‘laparoscopically experienced’; having more than 3 previous laparoscopic experiences constituted ‘experienced’ in one study [16] whereas participants with up to 750 laparoscopic cases logged were classed as ‘experienced’ in another [25]. At review level, the exclusion of non-English language studies may have increased the risk of language bias. However, strengths of the review include its comprehensive search strategy of numerous databases, adherence to the PRISMA [9] and SWiM [13] checklists, thorough quality assessment and its nature as the first systematic review investigating skill transfer of these modalities.
Implications for research and/or practice
All studies in the simulated setting assessed only the initial phase of the robotic surgery learning curve where skill transfer is most evident [37], so increasing the numbers of trials up to the acquisition of proficiency [23] in future studies would enable evaluation of skill transfer in the context of the whole learning curve. Given the reported additive mechanism by which a combination of virtual reality and augmented reality simulators enhance robotic performances [24], high-quality randomised controlled trials evaluating their impact on the robotic surgery learning curve are warranted especially as they can be adapted for use with robotic training modules [24] which may enable development of more cost-effective robotic surgery training curricula. Some studies also evaluated a robotic transfer effect to laparoscopy [20, 27, 32, 33, 38, 42] with contradictory findings, so further investigation of the impact of concomitantly teaching open, laparoscopic and robotic skills on trainee performances across the various modalities may aid in the development of more effective curricula to accelerate skill acquisition. Cohort studies with larger groups of surgeons in the intraoperative setting will enable more confident conclusions to be drawn regarding open and laparoscopic skill transfer in the clinical setting.
Regarding clinical practice, although all clinical studies [14,15,16,17] concluded that robotic skills can be acquired in the absence of any laparoscopic experience, open and laparoscopic training remains an essential part of robust surgical training. Robotic surgeons still employ laparoscopic skills such as pneumoperitoneum creation and adhesiolysis to facilitate port insertion [49], and they must be well-versed in open surgical techniques given the rates of conversion from robotic to open being as high as 9.2% for nephroureterectomy, for example [50]. Undergoing concomitant training across all modalities enables trainees to become more clinically skilled surgeons, able to safely and effectively undertake a variety of procedures thereby increasing the range of care they can provide. With results suggesting that laparoscopic skill transfer occurs in the initial phase of the learning curve, there is need for individually tailored curricula correlating with the level of laparoscopic expertise the trainee has.
Conclusion
Skill transfer from both modalities appears to be most apparent when advanced robotic tasks are performed in the initial phase of the learning curve but quality and methodological limitations of the existing literature prevent definite conclusions from being drawn. The impact of incorporating laparoscopic simulation into robotic training curricula on all phases of the robotic surgery learning curve and on the cost effectiveness of training should be investigated.
References
Lam K, Clarke J, Purkayastha S, Kinross JM (2021) Uptake and accessibility of surgical robotics in England. Int J Med Rob Comput Assist Surg 17(1):e2174
Lanfranco AR, Castellanos AE, Desai JP, Meyers WC (2004) Robotic surgery: a current perspective. Ann Surg 239(1):14–21
Cao L, Yang Z, Qi L, Chen M (2019) Robot-assisted and laparoscopic vs open radical prostatectomy in clinically localized prostate cancer: perioperative, functional, and oncological outcomes: a Systematic review and meta-analysis. Medicine (Baltimore) 98(22):e15770
Skupin PA, Stoffel JT, Malaeb BS, Barboglio-Romo P, Ambani SN (2020) Robotic versus open ureteroneocystostomy: is there a robotic benefit? J Endourol 34(10):1028–1032
Brook N, Dell’Oglio P, Barod R, Collins J, Mottrie A (2019) Comprehensive training in robotic surgery. Curr Opin Urol 29(1):1–9
Moglia A, Ferrari V, Morelli L, Ferrari M, Mosca F, Cuschieri A (2016) A systematic review of virtual reality simulators for robot-assisted surgery. Eur Urol 69(6):1065–1080
Li MM, George J (2017) A systematic review of low-cost laparoscopic simulators. Surg Endosc 31(1):38–48
Hertz AM, George EI, Vaccaro CM, Brand TC (2018) Head-to-head comparison of three virtual-reality robotic surgery simulators. JSLS J Soc Laparoendosc Surg 22(1):e201700081
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009(339):b2535
Chahal B, Aydin A. The transfer of open and laparoscopic surgical skills to robotic surgery: a systematic review PROSPERO 2021 CRD42021231235. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021231235, Accessed 15 Mar 2021
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng H-Y, Corbett MS, Eldridge SM, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:l4898
Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JPT (2016) ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ 355:i4919
Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S et al (2020) Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ 368:l6890
Ahlering TE, Skarecky D, Lee D, Clayman RV (2003) Successful transfer of open surgical skills to a laparoscopic environment using a robotic interface: initial experience with laparoscopic radical prostatectomy. J Urol 170(5):1738–1741
Eddib A, Jain N, Aalto M, Hughes S, Eswar A, Erk M et al (2013) An analysis of the impact of previous laparoscopic hysterectomy experience on the learning curve for robotic hysterectomy. J Robot Surg 7(3):295–299
Kilic GS, Walsh TM, Borahay M, Zeybek B, Wen M, Breitkopf D (2012) Effect of residents’ previous laparoscopic surgery experience on initial robotic suturing experience. ISRN Obstet Gynecol 2012:569456
Kim IK, Kang J, Park YA, Kim NK, Sohn SK, Lee KY (2014) Is prior laparoscopy experience required for adaptation to robotic rectal surgery? Feasibility of one-step transition from open to robotic surgery. Int J Colorectal Dis 29(6):693–699
Anderberg M, Larsson J, Kockum CC, Arnbjörnsson E (2010) Robotics versus laparoscopy—an experimental study of the transfer effect in maiden users. Ann Surg Innov Res 4:1–6
Angell J, Gomez MS, Baig MM, Abaza R (2013) Contribution of laparoscopic training to robotic proficiency. J Endourol 27(8):1027–1031
Ashley CW, Donaldson K, Evans KM, Nielsen B, Everett EN (2019) Surgical cross-training with surgery naive learners: implications for resident training. J Surg Educ 76(6):1469–1475
Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS (2007) Comparison of learning curves and skill transfer between classical and robotic laparoscopy according to the viewing conditions: implications for training. Am J Surg 194(1):115–121
Cumpanas AA, Bardan R, Ferician OC, Latcu SC, Duta C, Lazar FO (2017) Does previous open surgical experience have any influence on robotic surgery simulation exercises? Wideochirurgia I Inne Techniki Maloinwazyjne 12(4):366–371
Davila DG, Helm MC, Frelich MJ, Gould JC, Goldblatt MI (2017) Robotic skills can be aided by laparoscopic training. Surg Endosc Other Intervent Techn. 32:1–6
Feifer A, Al-Almari A, Kovacs E, Delisle J, Carrier S, Anidjar M (2010) Randomized controlled trial of virtual reality and hybrid simulation for robotic surgical training. J Urol 183(4):e423
Finnerty BM, Afaneh C, Aronova A, Fahey TJ, Zarnegar R (2016) General surgery training and robotics: are residents improving their skills? Surg Endosc 30(2):567–573
Hagen ME, Wagner OJ, Inan I, Morel P (2009) Impact of IQ, computer-gaming skills, general dexterity, and laparoscopic experience on performance with the da Vinci® surgical system. Int J Med Rob Comput Assist Surg 5(3):327–331
Hassan SO, Dudhia J, Syed LH, Patel K, Farshidpour M, Cunningham SC et al (2015) Conventional laparoscopic vs robotic training: which is better for Naive users? A randomized prospective crossover study. J Surg Educ 72(4):592–599
Jayaraman S, Quan D, Al-Ghamdi I, El-Deen F, Schlachta CM (2010) Does robotic assistance improve efficiency in performing complex minimally invasive surgical procedures? Surg Endosc 24(3):584–588
Kim HJ, Choi G-S, Park JS, Park SY (2014) Comparison of surgical skills in laparoscopic and robotic tasks between experienced surgeons and novices in laparoscopic surgery: an experimental study. Ann Coloproctol 30(2):71–76
Kowalewski KF, Schmidt MW, Proctor T, Pohl M, Wennberg E, Karadza E et al (2018) Skills in minimally invasive and open surgery show limited transferability to robotic surgery: results from a prospective study. Surg Endosc 32(4):1656–1667
McVey R, Goldenberg MG, Bernardini MQ, Yasufuku K, Quereshy FA, Finelli A et al (2016) Baseline laparoscopic skill may predict baseline robotic skill and early robotic surgery learning curve. J Endourol 30(5):588–593
Moncayo S, Compagnon R, Caire F, Grosos C, Bahans C, Ilhero P et al (2019) Transition effects from laparocscopic to robotic surgery skills in small cavities. J Rob Surg. 14:525–530
Obek C, Hubka M, Porter M, Chang L, Porter JR (2005) Robotic versus conventional laparoscopic skill acquisition: implications for training. J Endourol Endourol Soc 19(9):1098–1103
Panait L, Shetty S, Shewokis PA, Sanchez JA (2014) Do laparoscopic skills transfer to robotic surgery? J Surg Res 187(1):53–58
Passerotti CC, Franco F, Bissoli JCC, Tiseo B, Oliveira CM, Buchalla CAO et al (2015) Comparison of the learning curves and frustration level in performing laparoscopic and robotic training skills by experts and novices. Int Urol Nephrol 47(7):1075–1084
Pimentel M, Cabral RD, Costa MM, Neto BS, Cavazzola LT (2018) Does previous laparoscopic experience influence basic robotic surgical skills? J Surg Educ 75(4):1075–1081
Teishima J, Hattori M, Inoue S, Ikeda K, Hieda K, Miyamoto K et al (2012) Impact of laparoscopic experience on the proficiency gain of urologic surgeons in robot-assisted surgery. J Endourol 26(12):1635–1638
Thomaier L, Orlando M, Abernethy M, Paka C, Chen CCG (2017) Laparoscopic and robotic skills are transferable in a simulation setting: a randomized controlled trial. Surg Endosc 31(8):3279–3285
Tillou X, Collon S, Martin-Francois S, Doerfler A (2016) Robotic surgery simulator: elements to build a training program. J Surg Educ 73(5):870–878
Vurgun N, Vongsurbchart T, Myszka A, Richter P, Rogula T (2020) Medical student experience with robot-assisted surgery after limited laparoscopy exposure. J Robot Surg 15:443–450
Yoo B, Kim J, Cho J, Shin J, Lee D, Kwak J et al (2015) Impact of laparoscopic experience on virtual robotic simulator dexterity. J Minim Access Surg 11(1):68–71
Zihni A, Ge T, Ray S, Wang R, Liang Z, Cavallo JA et al (2016) Transfer and priming of surgical skills across minimally invasive surgical platforms. J Surg Res 206(1):48–52
Azadi S, Green IC, Arnold A, Truong M, Potts J, Martino MA (2021) Robotic surgery: the impact of simulation and other innovative platforms on performance and training. J Minim Invasive Gynecol 28(3):490–495
Schmidt MW, Köppinger KF, Fan C, Kowalewski KF, Schmidt LP, Vey J, Proctor T, Probst P, Bintintan VV, Müller-Stich BP, Nickel F (2021) Virtual reality simulation in robot-assisted surgery: meta-analysis of skill transfer and predictability of skill. BJS Open 5(2):zraa066
Lyons C, Goldfarb D, Jones SL, Badhiwala N, Miles B, Link R et al (2013) Which skills really matter? Proving face, content, and construct validity for a commercial robotic simulator. Surg Endosc 27(6):2020–2030
Hagen ME, Meehan JJ, Inan I, Morel P (2008) Visual clues act as a substitute for haptic feedback in robotic surgery. Surg Endosc 22(6):1505–1508
Hernandez JD, Bann SD, Munz Y, Moorthy K, Datta V, Martin S et al (2004) Qualitative and quantitative analysis of the learning curve of a simulated surgical task on the da Vinci system. Surg Endosc 18(3):372–378
Hvolbek AP, Nilsson PM, Sanguedolce F, Lund L (2019) A prospective study of the effect of video games on robotic surgery skills using the high-fidelity virtual reality RobotiX simulator. Adv Med Educ Pract 10:627–634
Sridhar AN, Briggs TP, Kelly JD, Nathan S (2017) Training in robotic surgery-an overview. Curr Urol Rep 18(8):58
Khanna A, Campbell SC, Murthy PB, Ericson KJ, Nyame YA, Abouassaly R (2020) Unplanned conversion from minimally invasive to open kidney surgery: the impact of robotics. J Endourol 34(9):955–963
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Baldev Chahal planned the review, performed the search strategies, extracted the data and wrote the manuscript. Mohammad S.A. Amin acted as second reviewer and contributed to writing the manuscript. Abdullatif Aydin acted as third reviewer, aided in planning of the review, and edited and reviewed the final manuscript. Kelly Ong, Azhar Khan, Muhammad S. Khan, Kamran Ahmed and Prokar Dasgupta provided revisions to the content of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Baldev Chahal, Abdullatif Aydin, Mohammad S.A. Amin, Kelly Ong, Azhar Khan, Muhammad S. Khan and Kamran Ahmed have no conflicts of interest or financial ties to disclose. Prokar Dasgupta declares financial ties with Proximie and MysteryVibe.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chahal, B., Aydın, A., Amin, M.S.A. et al. Transfer of open and laparoscopic skills to robotic surgery: a systematic review. J Robotic Surg 17, 1207–1225 (2023). https://doi.org/10.1007/s11701-022-01492-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-022-01492-9